In June of 2020, at the height of the COVID-19 pandemic and in light of an alarming rate of infection among Black people in the US, at an Ohio Senate Health and Human Services committee hearing, state Senator and emergency room Doctor Stephen Huffman inquired, in a problematic manner, why the rate of COVID was so high among Black people in the United States. He asked: “could it just be that African Americans or the colored population do not wash their hands as well as other groups? Or wear masks? Or do not socially distance themselves?” (Dickinson et al. 2021).
Source: NBC news
Such racial biases pervade the American medical system. Medical education centers white, male bodies and insufficiently investigates the underlying social factors that lead to higher rates of illness among people of color (Dickinson et al. 2021).
Currently, the national mortality rate for Black Americans is 2.1 times higher than that of Whites (Johnson-Agbakwu et al. 2022). Black people have 1.4 times higher rates of infection, 3.7 times higher hospitalization rates, and 2.8 higher death rates from COVID than White Americans (Dickinson et al. 2021). The Black American life expectancy before COVID-19 was 74. Since the start of the pandemic, life expectancy has dropped by another 2.1 years to 72 (Sederstrom and Lasege 2022).
Racist Explanations
In light of such health discrepancies, powerful figures, such as Dr. Stephen Huffman, all too quickly turn to racist explanations that echo debunked racist theories that blame communities of color.
Similarly to Dr. Huffman, during a press briefing in April 2020, US Surgeon General Jerome Adams, a Black American, perpetuated racial stereotypes when he encouraged communities of color to “step up” and “avoid alcohol, tobacco, and drugs,” adding: “Do it for your abuela, do it for your granddaddy, do it for your big momma, do it for your pop-pop. We need you to understand, especially in communities of color” (Dickinson et al. 2021).
Stereotypes and internal biases against African Americans have been used by many Americans to explain their higher rates of death due to COVID-19. National data shows that 56% of White people believe that Black people prefer to live off welfare, 29% view Black people as unintelligent, and 44% view them as lazy (Williams and Rucker 2000).
Despite the stereotype that Black people are less likely to wear masks, studies show that Black respondents were 8% more likely to wear masks compared with White respondents, while controlling for other socio-demographic factors (Dickinson et al. 2021). This is also despite the fact that, compared to 1% of White and Asian respondents, 8% of Black respondents voiced concerns of police brutality while wearing a mask at a time when Black Americans account for 28% of the people killed by the police (Dickinson et al. 2021).
Structural Racism Increases Health Risks
Higher COVID rates among Black people in America were tied to a host of underlying structural and enduring inequalities that persisted long after the Jim Crow era: these forces, not personal choices, likely gave rise to racial gaps in COVID rates.
Employment
A study analyzing health outcomes during the pandemic suggests that Black people have significantly lower household income than White people on average, and higher rates of having to go to work in-person weekly. 44% of Black respondents, compared with 29% of White respondents, said that they had to work outside their home. Black respondents also reported having to take public transportation 5 or more times within the 2 months prior to the study during the pandemic (Dickinson et al. 2021). These factors explain why non-white groups had higher exposure to COVID than White respondents.
Housing
Housing also placed African Americans at a disadvantage during the pandemic. The federal government created the Federal Housing Administration in 1933, which subsidized housing in areas where White people, but not people of color tended to live. Under this policy of “redlining,” African Americans were pushed into segregated neighborhoods which in turn have less economic investment, fewer resources, and more pollution and noise (Yearby and Mohapatra 2020). It also leads to higher rates of poverty in these areas giving residents less access to healthcare (Swope et al. 2022).
Overcrowded housing leads to higher rates of other health problems such as asthma, obesity, and cardiovascular disease which makes African Americans more susceptible to contracting COVID-19 (Yearby and Mohapatra 2020). With little resources within these segregated neighborhoods, African American, Latino households, and Native American households are almost twice as likely to ‘lack complete plumbing.’ Without plumbing, racial and ethnic minorities may struggle to maintain sanitary conditions that aid prevention of COVID-19 transmission (Yearby and Mohapatra 2020).
Additionally, on average, White respondents live in households with 0.6 to 0.7 less people than Black households (Dickinson et al. 2021). Larger households increase exposure and the spread of sickness, such as COVID-19, faster.
Healthcare
Structural racism also puts Black people at a disadvantage in receiving healthcare.
Current laws and policies, such as the Hill-Burton Act and the Kerr-Mills program, allocate resources such as health insurance to White populations. The Hill-Burton Act provides for construction of public hospitals and long term care facilities, but allows states to construct racially separate and unequal facilities (Yearby et al. 2022). The Kerr-Mills program, which provided healthcare to the poor, was underfunded and few states participated.
The Federal government has enacted a number of laws such as the Labor Relations Act of 1935 that expanded union rights for workers, including higher wages and benefits such as health insurance for those represented by unions. However, this doesn’t apply to service, domestic, and agricultural industries and it allowed unions to discriminate against racial and ethnic minority workers.
Inadequate health insurance coverage is one of the largest barriers in health care access with studies showing that low income minorities with bad health had 68% less odds of being insured than high income White people with good health. As of 2019, 58% of Americans were covered by employer-sponsored health insurance, with 66% of White workers covered by this insurance compared with 47% of Black (Yearby et al. 2022).
In conclusion, life circumstances of African Americans, influenced by a legacy of structural racism, placed them at a disadvantage during the COVID-19 pandemic. Decades of redlining led to disinvestment in crucial areas such as housing, transportation, and education, which as a result, led Black respondents to reside in larger households, work in lower-paying public-facing roles, and rely on public transportation, all of which are structural factors that heighten the risk of COVID-19 exposure.
Countering Structural Racism
In order to address racism within the healthcare system and raise awareness of other racial inequities across everyday life in the United States, institutional policies should mandate training across clinicians and other health care professionals about the roots of structural racism. Health care professionals should also reflect on their own internal implicit biases and how to approach their careers in an equitable manner through processes such as the transformative learning theory (TLT).
TLT suggests that learning involves a process triggered by disruption, followed by a revised interpretation of experiences that guide an individual’s actions. It requires experience, critical reflection, dialogue, and action (Sukhera et al. 2020). A trigger often used to spark awareness of implicit bias is the Implicit Association Test which was developed by Drs Mahzarin Banaji and Anthony Greenwald to measure unconscious bias (Marcelin et al. 2019). 75% of test takers demonstrate an automatic White preference (Marcelin et al. 2019). Through TLT, health professionals can become aware of their implicit biases and engage in dialogue to help them transform.
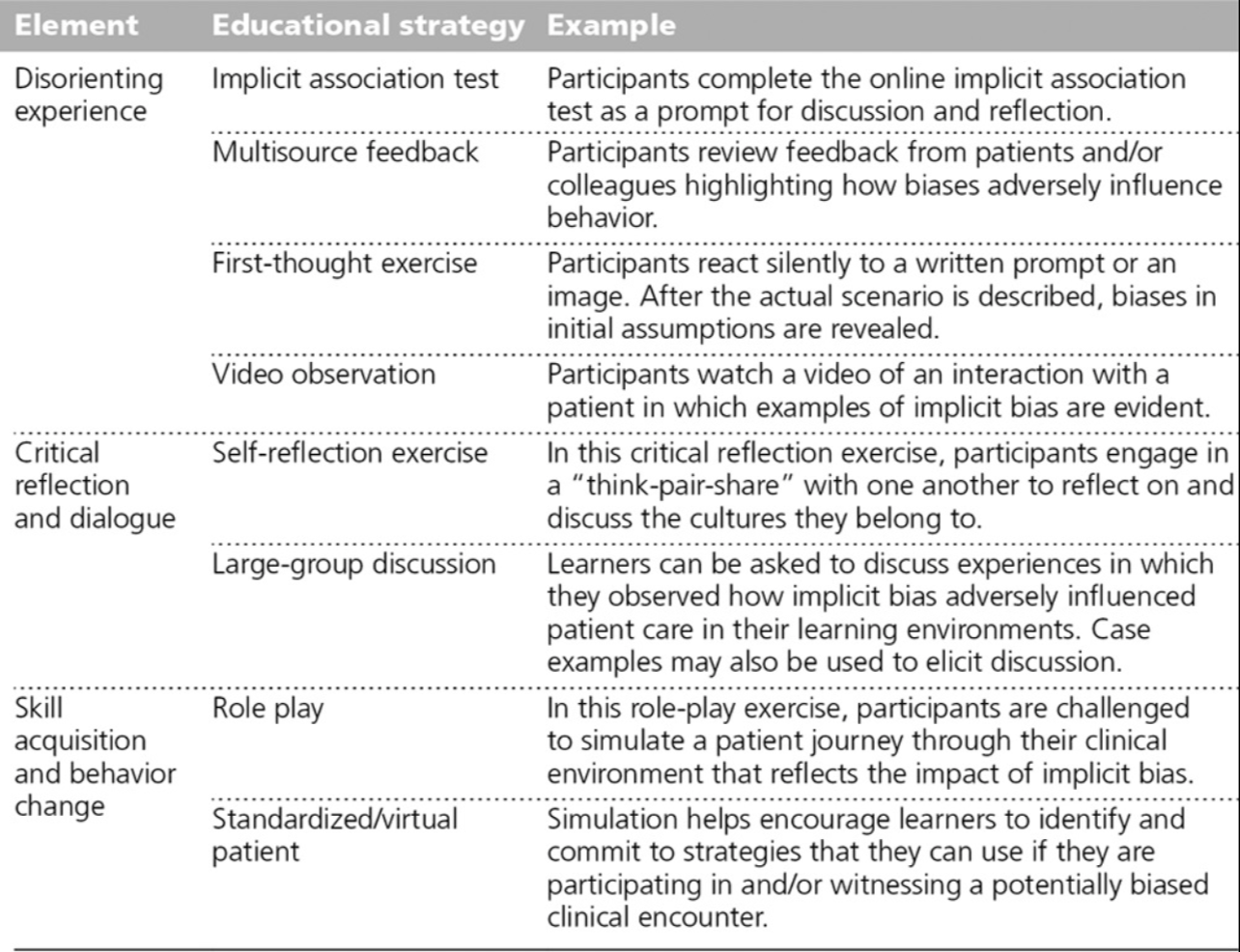
Source: (Sukhera et al., 2020)
The goals of transformative learning are to increase awareness of how we construct reality and to break free from the limiting structures that shape our understanding of our experiences (Sukhera et al., 2020).
Efforts should be made to recruit diverse faculty and staff and ensure there is representation throughout all levels of leadership. Studies show that communities of color receive better care when cared for by providers who share their racial and cultural identity (Johnson-Agbakwu et al. 2022). Black Americans, however, represent 12% of the US population but only 5% of US medical professionals (Johnson-Agbakwu et al. 2022), stemming from the structural racism that puts people at a disadvantage in living conditions and access to education. In fostering diversity and inclusion within the medical profession, systemic inequalities can be addressed and advancements can be made towards a healthcare system that better serves all individuals, regardless of their race or cultural background.
Works Cited
Dickinson, K. L., Roberts, J. D., Banacos, N., Neuberger, L., Koebele, E., Blanch-Hartigan, D., & Shanahan, E. A. 2021. “Structural Racism and the COVID-19 Experience in the United States.” Health Security, S-14-S-26. http://doi.org/10.1089/hs.2021.0031
Hill, J. L., & Hamilton, D. 2020. “The color of coronavirus: COVID-19 deaths by race and ethnicity in the U.S.” Harvard Data Science Review, 2(1). https://doi.org/10.1162/99608f92.8cd55085
Johnson-Agbakwu, C.E., Ali, N.S., Oxford, C.M. 2022. “Racism, COVID-19, and Health Inequity in the USA: a Call to Action.” Journal of Racial and Ethnic Health Disparities, 9(1), 52–58. https://doi.org/10.1007/s40615-020-00928-y
Marcelin, R. J., Siraj, S. D., Victor, R., Kotadia, S., Maldonado, A. Y. 2019. “The Impact of Unconscious Bias in Healthcare: How to Recognize and Mitigate It.” The Journal of Infectious Diseases, S62-S73. https://academic.oup.com/jid/article/220/Supplement_2/S62/5552356
Sukhera, J., Watling, C., Gonzalez, C. 2020. “Implicit Bias in Health Professions: From Recognition to Transformation.” Journal of the Association of American Medical Colleges, 95(5), 717-723. https://journals.lww.com/academicmedicine/fulltext/2020/05000/implicit_bias_in_health_professions__from.21.aspx
Swope, B. C., Hernández, D., Cushing, J. L. 2022. “The Relationship of Historical Redlining with Present-Day Neighborhood Environmental and Health Outcomes: A Scoping Review and Conceptual Model.” Journal of Urban Health, 959-983. https://link.springer.com/article/10.1007/s11524-022-00665-z
Williams, R. D., Rucker, D. T. 2000. “Understanding and Addressing Racial Disparities in Healthcare.” National Library of Medicine, 21(4), 75-90. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4194634/
Yearby, R., Clark, B., Figueroa, F. J. 2022. “Structural Racism In Historical And Modern US Health Care Policy.” Health Affairs, 41(2). https://www.healthaffairs.org/doi/full/10.1377/hlthaff.2021.01466
Yearby, R., Mohapatra, S. 2020. “Law, structural racism, and the COVID-19 pandemic.” Journal of Law and the Biosciences, 1-20. https://watermark.silverchair.com